Crohn’s Disease doesn’t just affect the gut. Up to 1 in every 2 people with Crohn’s develop problems in other parts of the body. Commonly affected areas include joints, eyes, and skin. These are known as extraintestinal manifestations or EIMs. They usually happen during a flare-up, but can occur without or before any gut symptoms.
For many of the complications, there are things you can do to reduce your risk.
Joints
Joint pain or swelling is common problem for people with Crohn’s. For some, this will get worse during a flare-up, but will usually improve with treatment for Crohn’s. Others may have joint problems even when gut symptoms feel better. Find out more in our information on joints.
Bones
People with Crohn’s are more at risk of developing thinner and weaker bones, known as osteoporosis. This can be due to ongoing inflammation, smoking, taking steroids or low levels of physical activity. Calcium is needed for bone formation, and this may be low if your diet doesn’t contain enough dairy. Weight-bearing exercise, calcium and vitamin D supplements, not smoking and avoiding long-term steroid use can help. For some people, medicines can be helpful. Find out more in our information on bones.
Skin
Crohn’s can affect the skin in different parts of the body.
Erythema nodosum affects between four and fifteen in every 100 people with Crohn’s. It causes raised, painful patches of skin that look red or darker than the surrounding skin. It is often found on the legs. It usually occurs during flare-ups and usually improves with treatment for Crohn’s.
Pyoderma gangrenosum starts as small tender blisters or pustules, which become painful, deep ulcers. On brown or black skin, the skin around the edge of the ulcer might be darker. Pyoderma gangrenosum can occur anywhere on the skin, but most commonly appear on the legs, or near stomas. This condition is sometimes linked to a flare-up. It’s often treated with steroids or biologic medicines. In some cases a specialist in skin conditions, called a dermatologist, may treat this with creams or ointments.
Sweet syndrome is where tender red lumps appear on the upper limbs, face, and neck, sometimes with a fever. The colour of the lumps can differ depending on skin tone. They may look red, pink, purple or dark brown in colour. It is generally associated with active Crohn’s. Doctors often use steroids or immunosuppressants to treat Sweet syndrome.
Other skin conditions that may be associated with Crohn’s include:
- Psoriasis. This is raised patches of flaky skin which forms scales. It usually appears on your elbows, knees, scalp and lower back.
- Rosacea. A condition causing redness, most commonly on your cheeks or nose. Redness may be harder to see on black or brown skin.
- Hidradenitis suppurativa. This is where lumps grow on the surface of the skin, usually around the armpits, bottom, groin and genitals. The lumps are often painful and can sometimes leak pus.
Eyes
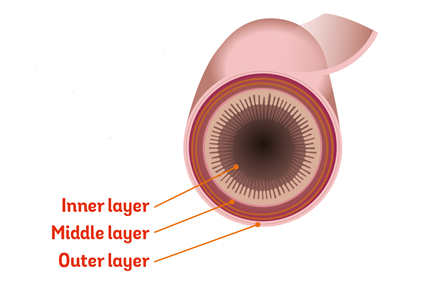
Episcleritis affects the layer of tissue covering the white outer coating of the eye, called the sclera. Your eyes become red, itchy and sometimes painful. This tends to flare up at the same time as Crohn’s symptoms. It often gets better with treatment for Crohn’s or with steroid eye drops.
Uveitis is inflammation of the iris and scleritis is inflammation of the sclera. These are serious and can lead to loss of vision if they’re not treated. Symptoms include pain, changes in vision and sensitivity to light. They’re treated with steroid drops, and sometimes immunosuppressants or biologic medicines.
These conditions are not to be confused with conjunctivitis, a common eye condition that is not associated with Crohn’s or Colitis. Conjunctivitis causes redness and irritation and produces sticky pus.
If you get any kind of painful eye irritation, redness or inflammation, tell your healthcare professional. They may refer you to an eye specialist.
Mouth
Some people with Crohn’s may develop mouth ulcers during flare-ups. These are painful, shallow, round and can be found on the smooth surfaces inside the mouth or under the tongue.
Kidneys
Kidney stones may be caused by:
- Inflammation in the small bowel, which can stop you absorbing enough fat. The fat is then left in the bowel and binds to calcium, forming a molecule called oxalate. This may be absorbed and deposited in the kidneys where it can form stones.
- You may become dehydrated if you lose fluid through diarrhoea and this can lead to kidney stones.
- Symptoms of kidney stones include pain, feeling sick, being sick and blood in your pee. Find out more on the NHS website.
Liver
Gallstones. People with Crohn’s are more likely to develop gallstones, with up to 1 in 3 people affected. Gallstones are small stones made of cholesterol. These may get trapped in the gallbladder and can be very painful.
Gallstones are more likely if:
- The end of the small bowel has been removed.
- There is severe inflammation in the small bowel.
Primary Sclerosing Cholangitis (PSC). This is a rare condition that affects around 1 in 50 people with Inflammatory Bowel Disease. It causes inflammation of the bile ducts and can eventually damage the liver. Symptoms include fatigue, itching, weight loss and jaundice, where your skin and whites of your eyes turn yellow. Talk to your IBD team if you are worried about any of these symptoms.
Circulation
Blood clots. You’re more likely to develop blood clots if you have Crohn’s. This includes deep vein thrombosis, known as DVT, in the legs and pulmonary embolisms, known as PE, in the lungs.
You’re more at risk:
- During a flare-up.
- If you have recently had surgery.
- If you need to stay in bed, for example in hospital.
To lower your risk:
- Don’t smoke.
- Stay active. Activities such as walking can help.
- Drink plenty of fluids to avoid dehydration.
These precautions can also be helpful when you travel by plane, car or train for more than three hours, which increases the risk of blood clots for everyone. Find out more in our information on travel.
If you’re staying in hospital because you’re unwell with your Crohn’s, you should be offered a medicine or injections to prevent blood clots.
Cardiovascular disease
People with active Crohn’s may have a slightly increased risk of cardiovascular disease, including heart problems and strokes.
Anaemia. If you’re anaemic, you have fewer red blood cells than normal and/or lower levels of haemoglobin in your blood. Haemoglobin is a protein found in red blood cells that carries oxygen around the body. There are several types of anaemia. People with Crohn’s are likely to develop iron deficiency anaemia. It is caused by a lack of iron in your diet, poor absorption of iron from food, or blood loss from the gut.
Anaemia can make you feel very tired. If it’s more severe you may also have shortness of breath, headaches, and general weakness.
Treatment depends on the cause of anaemia. You may be prescribed iron supplements that are taken by mouth. Or you may be given iron into your vein by an injection or infusion through a drip. Find out more about iron in our information on other treatments.
Hair loss
You might lose more hair if you have Crohn’s. This could be due to a condition called alopecia areata or a condition called telogen effluvium. Both are associated with Crohn’s and Colitis.






 Become a member: Find out about the benefits of joining our amazing community
Become a member: Find out about the benefits of joining our amazing community