
Help us improve our information
We need your help to improve our information to better support people with Crohn’s and Colitis. Fill in our short survey to let us know what we're doing well and how we can better meet your needs.
Biologics and other targeted medicines are types of treatment for Crohn’s and Colitis. In general, they are prescribed for people with moderate to severe Crohn's or Colitis.
This information provides an overview of biologics and other targeted medicines. It is for people who may be starting treatment with one, or considering it as an option.
It looks at:
This information might use words you have not heard before. Our page on medical words can help provide an explanation.
We have separate, detailed information about each of the individual medicines used to treat Crohn’s and Colitis.

We need your help to improve our information to better support people with Crohn’s and Colitis. Fill in our short survey to let us know what we're doing well and how we can better meet your needs.
Your IBD team should review your treatment at least once a year to check that it is still the right option for you.
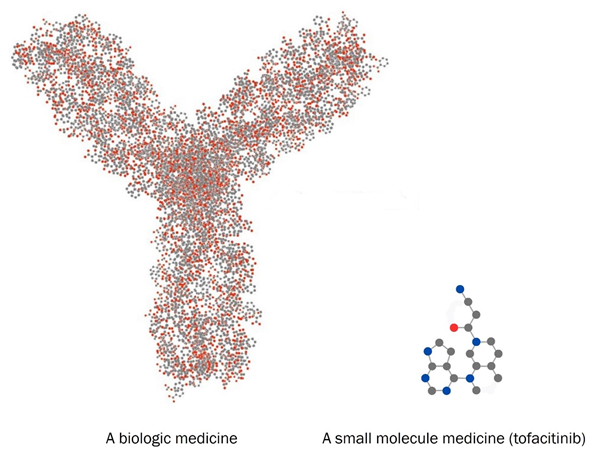
Crohn’s Disease and Ulcerative Colitis cause inflammation in your gut, and sometimes other parts of your body. Biologics and other targeted medicines are treatments that block particular proteins or chemical pathways involved in inflammation. This reduces inflammation. They are more precise than immunosuppressant medicines.
The pathways that biologics and other targeted medicines block are part of your immune system. So these medicines can affect the way your immune system works. This means your body might not fight off infections as well as other people. You might get more infections than you used to, or they might last longer or be more serious than usual.
Biologics and other targeted medicines may be an option for people with moderate to severe Crohn’s Disease or Ulcerative Colitis:
They are often considered:
They might also be used as a first medicine if your IBD team feel they are the best option for you. They may be especially useful in people with severe Crohn’s or Colitis or people who also have non-gut symptoms or fistulas.
Lots of biologics and other targeted medicines are available in the UK to treat Crohn’s and Colitis. Some are used to treat Crohn’s, some to treat Colitis, and some to treat both. Sometimes they can only be used in particular circumstances, like when other options have not worked. Not all medicines are suitable for everyone.
Sometimes, your IBD team might suggest using medicines outside their licensed indications if they appear to be the best available option for you.
Below, we give an overview of biologics that are currently available in the UK. More are being developed and could be available in the future.
We also have separate detailed information on individual medicines.
Brand names: Amgevita, Hyrimoz, Idacio, Imraldi, Humira, Yuflyma.
Used to treat: Crohn’s Disease or Ulcerative Colitis in adults and children over 6.
How it works: It is a type of medicine called an anti-TNF. It sticks to a protein called TNF-alpha. Your immune system naturally makes TNF to help you fight infections, but it can also cause inflammation. Adalimumab blocks the effects of TNF-alpha, which helps reduce inflammation.
Full drug information available at: Adalimumab
Brand names: Simponi.
Used to treat: Ulcerative Colitis in adults.
How it works: It is a type of medicine called an anti-TNF. It sticks to a protein called TNF-alpha. Your immune system naturally makes TNF to help you fight infections, but it can also cause inflammation. Golimumab blocks the effects of TNF-alpha, which helps reduce inflammation.
Full drug information available at: Golimumab
Brand names: Flixabi, Inflectra, Remicade, Remsima, Zessly.
Used to treat: Crohn’s Disease (including fistulas) or Ulcerative Colitis in adults and children over 6.
How it works: It is a type of medicine called an anti-TNF. It sticks to a protein called TNF-alpha. Your immune system naturally makes TNF to help you fight infections, but it can also cause inflammation. Infliximab blocks the effects of TNF-alpha, which helps reduce inflammation.
Full drug information available at: Infliximab
Brand names: Omvoh.
Used to treat: Ulcerative Colitis in adults.
How it works: It is a type of medicine called an IL-23 inhibitor. It sticks to a protein called interleukin-23, or IL-23. Your immune system naturally makes IL-23 to help you fight infections, but it can also cause inflammation. Mirikizumab blocks the effects of IL-23, which helps reduce inflammation.
Full drug information available at: Mirikizumab
Brand names: Skyrizi.
Used to treat: Crohn’s Disease in people over 16.
How it works: It is a type of medicine called an IL-23 inhibitor. It sticks to a protein called interleukin-23, or IL-23. Your immune system naturally makes IL-23 to help you fight infections, but it can also cause inflammation. Risankizumab blocks the effects of IL-23, which helps reduce inflammation.
Full drug information available at: Risankizumab
Brand names: Imuldosa, Otulfi, Pyzchiva, Stelara, Steqeyma, Uzprovo, Wenzela.
Used to treat: Crohn’s Disease or Ulcerative Colitis in adults.
How it works: It is a type of medicine called an IL-12/23 inhibitor. It sticks to two different proteins, called interleukin 12 and interleukin 23, or IL-12 and IL-23. Your immune system naturally makes these to help you fight infections, but they can also cause inflammation. Ustekinumab blocks the effects of IL-12 and IL-23, which helps reduce inflammation.
Full drug information available at: Ustekinumab
Brand names: Entyvio.
Used to treat: Crohn’s Disease or Ulcerative Colitis in adults.
How it works: It is a type of medicine called a gut-selective integrin blocker. It sticks to a protein called integrin on the surface of the white blood cells. This stops the white blood cells entering your gut, where they can cause inflammation.
Full drug information available at: Vedolizumab
Below, we give an overview of other targeted medicines that are currently available in the UK. More are being developed and could be available in the future.
We also have separate detailed information on individual medicines.
Brand names: Velsipity.
Used to treat: Ulcerative Colitis in adults.
How it works: It is a type of medicine called an S1P receptor modulator. It sticks to a protein called sphingosine-1-phosphate (S1P) on some white blood cells. This stops them from travelling into your gut and causing inflammation.
Full drug information available at: Etrasimod
Brand names: Jyseleca.
Used to treat: Ulcerative Colitis in adults.
How it works: It is a type of medicine called a JAK inhibitor. It blocks the effects of proteins called janus kinases, or JAKs. JAKs activate your immune system and help you fight infection, but they also cause inflammation. Blocking the effects of JAKs helps reduce gut inflammation.
Full drug information available at: Filgotinib
Brand names: Zeposia.
Used to treat: Ulcerative Colitis in adults.
How it works: It is a type of medicine called an S1P receptor modulator. It sticks to a protein called sphingosine-1-phosphate (S1P) on some white blood cells. This stops them from travelling into your gut and causing inflammation.
Full drug information available at: Ozanimod
Brand names: Xeljanz.
Used to treat: Ulcerative Colitis in adults.
How it works: It is a type of medicine called a JAK inhibitor. It blocks the effects of proteins called janus kinases, or JAKs. JAKs activate your immune system and help you fight infection, but they also cause inflammation. Blocking the effects of JAKs helps reduce gut inflammation.
Full drug information available at: Tofacitinib
Brand names: Rinvoq.
Used to treat: Crohn’s Disease or Ulcerative Colitis in adults.
How it works: It is a type of medicine called a JAK inhibitor. It blocks the effects of proteins called janus kinases, or JAKs. JAKs activate your immune system and help you fight infection, but they also cause inflammation. Blocking the effects of JAKs helps reduce gut inflammation.
Full drug information available at: Upadacitinib
Deciding to take a new medicine can feel like a big step. There are lots of things to think about. Your IBD team should discuss your options with you.
Some people worry about having injections or blood tests, taking time off work for treatment, or having a lowered immune system. But biologics and other targeted medicines can help get Crohn’s or Colitis under control and keep them under control.
My experience of having been on Humira, Remicade and Remsima are only positive, all can be life changing, and when they work it is like you no longer have IBD. Ensure you keep in contact with your IBD team and let them know how you are doing – remember they have lots of experience of IBD and are the best people to talk to.
Barry
Living with Crohn's Colitis
There are many different treatments available, and it can be difficult to predict which one will work best for you. Your IBD team might give you a choice of different treatments. You should consider the potential benefits, possible risks, and the goals of your treatment together.
Things to consider include:
Our Appointment guide includes a list of questions you might want to ask. It can help you focus on what matters most to you.
Before you start a biologic or other targeted medicine, your IBD team will ask you some questions and do some blood tests to make sure it’s suitable for you. They will also make sure your vaccinations are up to date. They may do a chest X-ray.
How you take your medicine depends on the type of medicine you are on.
You cannot take biologics by mouth because they are broken down in the gut, which stops them working. Instead you either have them as an infusion (a drip in your arm), or as an injection under your skin.
Depending on which medicine you are on, you might:
You could think about whether a hospital infusion or an injection at home would work best for you. It might be helpful to look at our Guide for employees and Guide for employers. These include information about taking time off for medical appointments.
Watch the video to find out what happens when you have an infusion.
You have some biologics as injections under your skin. This is called a subcutaneous injection.
Once you’ve got used to your medicine, your doctor or nurse will usually teach you how to give yourself the injection at home. This could be through an injection pen, a pre-filled syringe, or an injector that you stick to your skin (called an on-body injector).
A pre-filled syringe

An injection pen

An on-body injector

Injecting yourself might sound daunting at first, but most people find it a lot easier than they expected. If you’re not comfortable injecting yourself, your doctor or nurse might be able to teach a friend or family member to do it for you.
When I was first told I needed to inject myself at home, I was worried about doing it wrong. However, you have the support of a nurse to begin with to build up your confidence. Now my fortnightly injections feel like part of my routine - like brushing my teeth.
Sophie
Living with Crohn’s
If you have home injections, you usually have them sent straight to you by a homecare delivery service. You have to store biologic medicines in the fridge.
Other targeted medicines are tablets that you take by mouth. Depending on which medicine you are on, you take them once or twice a day.
If the first biologic or targeted treatment you try is not right for you, you may need to change to a different one. The decision about which treatment to try next depends on several factors. Your IBD team should discuss this with you and make the decision together.
There are a few reasons you may need to change treatment.
Biologics and other targeted medicines don’t work for everyone. Some people find that treatment does not help them feel better. Your IBD team will monitor how well your treatment is working.
If your symptoms do not improve within a few months, your IBD are likely to suggest stopping the medicine and trying a different option. Switching to a medicine that works in a different way could be an option.
For some people, treatment works well at first but stops working over time.
For biologic medicines, this can happen because your immune system recognises the drug as a foreign substance and thinks it is harmful. It then produces proteins called antibodies against the biologic drug, which stop it working as well.
If this happens there may be a few options:
Tell your IBD team if you are getting side effects. If you have side effects that are serious or hard to manage, they might suggest stopping treatment and trying a different option.
When you change to a different medicine, your IBD team might recommend taking a break from treatment for a few weeks. This is to make sure all the first medicine is out of your system before you start the next one. It is called a washout period. The idea behind it is to keep your risk of infection as low as possible, but the evidence on whether or not it is needed is unclear.
A recent study found no difference in infection risk in people who had a washout period of less than 30 days compared to people who had a washout period of more than 30 days. So you might not need to stop treatment for long. Your IBD team will tell you what they recommend.
Sometimes, your IBD team might suggest switching to a different brand of the same medicine. This could happen for a few reasons, such as:
Your IBD team will let you know if they are considering switching you to a different brand of medicine. This could be by letter, text, email, or at an appointment.
You should have a chance to discuss the switch and make the decision together. This should consider your needs, preferences and values as well as the clinical evidence.
For biologic medicines, different brands are slightly different from each other. This is because biologics are very complex medicines made by living cells, so it is not possible to make an exact copy. These slightly different brands are called biosimilars. They are very similar to the original medicine.
Biosimilars are thoroughly tested to make sure they are just as safe and effective as the original brand.
Biosimilars are much cheaper for the NHS than the original brand. The money saved means more people can access treatment. There is no evidence that switching to a biosimilar makes your Crohn’s or Colitis get worse or flare up.
However, there are likely to be some small differences between brands, including:
The Patients Association has more information on switching to biosimilars. This includes a video about biosimilars, and a biosimilars leaflet to download.
If you have any problems after switching brands, tell your IBD team.
Together you can agree the best way forward. Depending on your experience, they may suggest switching back to your original brand, or trying a different medicine.
Your IBD team should review your treatment at least once a year. If it is working and you are not getting serious side effects, they are likely to recommend that you carry on taking it. If you’re finding side effects hard to manage, or you want to have a break from treatment, tell your IBD team. They can help you consider your options.
If your Crohn’s or Colitis stays under control for a long time, your IBD team might suggest stopping your biologic or other targeted medicine. They should discuss it with you so you can make the decision together. You can tell them if you have any concerns about stopping. If you do stop treatment, your team will monitor you. If your symptoms come back, you should have the option to start treatment again.
If you’ve been taking a biologic or other targeted medicine with an immunosuppressant such as azathioprine, your IBD team might suggest taking the immunosuppressant alone.
We follow strict processes to make sure our information is based on up-to-date evidence and easy to understand.
Please email us at evidence@crohnsandcolitis.org.uk if:
You can also write to us at Crohn’s & Colitis UK, 1 Bishop Square, Hatfield, AL10 9NE, or contact us through our Helpline: 0300 222 5700
Use this tool to understand more about potential treatment options that suit your needs. The tool is designed to help you:
This page has been saved in your personal space. Go to “My Page” to view all saved pages.
We know it can be difficult to live with, or support someone living with these conditions. But you’re not alone. We provide up-to-date, evidence-based information and can support you to live well with Crohn’s or Colitis.
Our helpline team can help by:
Providing information about Crohn’s and Colitis.
Listening and talking through your situation.
Helping you to find support from others in the Crohn’s and Colitis community.
Providing details of other specialist organisations.
Please be aware we’re not medically or legally trained. We cannot provide detailed financial or benefits advice or specialist emotional support.
Please contact us via telephone, email or LiveChat - 9am to 5pm, Monday to Friday (except English bank holidays).
If you need specific medical advice about your condition, your GP or IBD team will be best placed to help.
Would you like to save the changes made to this page?
Your details were successfully saved.