
Help us improve our information
We need your help to improve our information to better support people with Crohn’s and Colitis. Fill in our short survey to let us know what we're doing well and how we can better meet your needs.
To find out if you have Crohn’s or Colitis, the two main forms of Inflammatory Bowel Disease (IBD), your doctor may offer you some medical tests and investigations. This information is for anyone who wants to find out more about the tests and investigations you might have. The results from these tests will help make sure that you are diagnosed correctly. The same tests help your doctors check (monitor) your health and find the best treatment for you.
This information might use words you have not heard before. Our page on medical words can help provide an explanation.
Talk to your doctor or IBD team for more detailed information about the tests. They will be happy to help with any queries or concerns. You may also find that your hospital or clinic has its own information on specific tests and investigations.
We know that getting a diagnosis or managing your condition can sometimes feel like an overwhelming process. We are here to help. Contact our helpline or visit our information pages for more information.
We need your help to improve our information to better support people with Crohn’s and Colitis. Fill in our short survey to let us know what we're doing well and how we can better meet your needs.
You will probably only need to have some of the tests listed in this information, and you are unlikely to have them all at once. Crohn’s and Colitis are fluctuating, ongoing conditions. This means your symptoms may come and go. So, it is likely that you will need to have some of the tests repeated from time to time.
The results from the tests I’ve had, have helped to keep me informed about how I am physically, which has really given me a feeling of being in control of my condition.
Bev
Living with Colitis
You may also have other tests that are not listed in our information. Symptoms of Crohn’s or Colitis can be similar to other bowel conditions. Other tests may be done to rule out other conditions.
If you think you might have Crohn’s or Colitis, the first thing to do is talk to your GP and read our information on how to get a diagnosis. Don’t be afraid to ask your GP specifically if they think it could be Crohn’s or Colitis. It could help to mention the Inflammatory Bowel Disease toolkit for GPs, which has guidance for when GPs should test for the conditions.
There is no one test to diagnose Crohn’s or Colitis. Your GP will consider all of your symptoms, together with your blood and poo test results. To confirm a diagnosis, your GP may send you to have endoscopies, scans or X-rays.
Crohn’s affects any part of the gut from your mouth to your bottom (anus). Colitis usually begins in the rectum and lower colon, but it may involve all of the large bowel.
Your GP will need to rule out other conditions, such as irritable bowel syndrome (IBS), coeliac disease, and bowel infections. You may need to see different specialists, including gastroenterologists and radiologists. It can take time to confirm a diagnosis of Crohn’s or Colitis.
Getting a diagnosis can be an overwhelming process. You may be feeling a mix of emotions during this time. You might feel frustrated at having to go to lots of different appointments. If you are diagnosed with Crohn’s or Colitis, you may feel relief that you’ve finally put a name to your symptoms and can start to manage them. Read our information on support for newly diagnosed people.
Our appointment guide can help you get the most out of your appointments and understand what matters most to you about your treatment and care. It will help you work together with your IBD team to find what’s right for you.
A lot of people don’t like blood tests - I know I didn’t at the beginning. But over time it does become easier to deal with.
Nicholas
Living with Colitis
A doctor or nurse will put a tight band (torniquet) around your arm to make your veins easier to see. They will gently put a needle into the vein, usually on the inside of your elbow or wrist. The nurse or doctor will collect a sample of your blood into a syringe or a small collecting container. The blood sample is then labelled and sent off for testing.
If you are worried about needles or seeing blood, let the doctor or nurse know. They can make sure you are as comfortable as possible and answer any questions you have.
Visit the NHS website to read more about what happens during a blood test.
For some specialised tests, you may be asked not to eat (fast) overnight or a few hours before the sample is taken. Your doctor or nurse will let you know if this is needed. Your doctor may ask for these tests to be repeated over time.
Several blood tests are used to help diagnose Crohn’s or Colitis. The doctor will look closely at the samples of your blood for different ‘markers’ or signs of Crohn’s and Colitis. They can also use these tests to check the level of certain cells, proteins, vitamins and minerals in your body. These tests can also help your doctor monitor your health and check whether the medicine you take for your Crohn’s or Colitis is causing any side effects.
After your blood sample has been checked or tested at a laboratory, your blood test results are usually sent back to your GP or hospital. Blood test results can take different times to come back. Some results will be ready the same day or the day after your blood test. And other results may take a couple of days or a few weeks to come back. When you have your test, you will be told roughly how long your results will take to come back and how you will be given them. Your results could be sent to you in a letter, discussed in person, be available to view on the NHS app (if you are signed up and linked to your GP) or on your GP’s online system.
When you read your blood test results, you might find your results are compared to a reference range. Reference ranges are based on the typical ‘normal’ test results of a large group of healthy people. We do not include the reference ranges for blood tests in our information as the ranges can depend on a number of factors, including the laboratory where the test was done, and sometimes your age and sex.
Blood test results can be difficult to understand, especially if there are many different results on one report, such as with a full blood count (FBC). Lab Tests Online have some information on reading your test results, including examples and the meanings of some of the words you might find in your results report. Ask your GP if you are unsure how to read your blood test results or want to know more about your results.
The blood tests used most often are:
A FBC measures the three main types of blood cells - red blood cells, white blood cells and platelets. It is used to check your general health and look for problems such as infections, anaemia and inflammation. Doctors talk about a ‘range’ of results since some people naturally have higher or lower levels than others.
A FBC looks for:
If you’re anaemic, you have fewer red blood cells than normal. The test to measure this is called a haemoglobin level. Haemoglobin is a protein found in red blood cells that carries oxygen around the body. Being anaemic can make you feel very tired. If it’s more severe, you might also develop shortness of breath, headaches, and general weakness. You may need to have a FBC test to check for anaemia every 3-12 months. This depends on if your Crohn’s or Colitis is active (such as during a flare-up) or in remission.
Some medicines used to treat Crohn’s and Colitis, such as azathioprine and mercaptopurine, can affect the bone marrow (where the body makes blood cells). If you are taking these medicines, your doctor may ask you to have a regular FBC to check your levels of red cells, white cells and platelets.
C-Reactive Protein (CRP) is a protein made by the liver that can be found in the blood. The level of CRP increases when there’s inflammation in your body. A CRP test is a blood test that measures the levels of these proteins (called inflammatory markers). If you have a higher level of CRP in your blood than usual, it could be a sign that you are in a flare-up or that treatment has not been effective. If the CRP level in your blood drops, it could be a sign that inflammation is reducing and your treatment is working.
CRP proteins are not only found in the gut. You may show a higher level of CRP if you have inflammation somewhere else in your body. Also, you may have inflammation in your body but show a normal level of CRP in your blood.
An LFT is a blood test that shows how well your liver is working. It can also help diagnose rare liver complications of Crohn’s or Colitis, such as Primary Sclerosing Cholangitis (PSC). PSC is a condition which causes the tubes (ducts) carrying bile from the liver to the gut to become inflamed.
An LFT measures the levels of enzymes (proteins that speed up chemical reactions in the body) made in your liver. These enzymes can leak into your blood when the liver is damaged.
An LFT also measures levels of albumin. Albumin is a protein made by the liver which helps keep blood flowing through your bloodstream. A low albumin level can be a sign of a problem with your liver but can also be due to inflammation in other parts of the body (such as the gut).
Some medicines used to treat Crohn’s and Colitis, such as azathioprine, can cause liver problems. Your doctor may ask you to have regular LFTs to check your liver is working properly.
Your doctor may do a blood test to check the levels of:
The amounts of electrolytes, urea and creatinine in the blood show how well your kidneys work. The tests can also check for dehydration (a common side effect of having frequent diarrhoea). Regular U&E tests are often recommended if you take some medicines to treat your Crohn’s or Colitis, especially mesalazine.
Levels of ferritin (and sometimes transferrin) in your blood are measured to diagnose iron deficiency anaemia. This blood test is usually done with a Full Blood Count.
Ferritin is the protein that stores iron in your body. Transferrin is the protein that moves iron around the body (carrying it away from the gut for storage and to the bone marrow to make red blood cells). Levels of ferritin and transferrin can show the total amount of iron stored in your body. Your doctor can use the ferritin and transferrin tests to tell if anaemia is caused by iron deficiency or another cause (such as chronic disease). People with Crohn’s or Colitis may have iron deficiency due to:
Vitamin B12 (also known as cobalamin) and vitamin B9 (commonly called folic acid) are both important for your health. They are vitamins that cannot be made in your body, so you need to get them from the food you eat.
Vitamin B12 and folic acid are used to make red blood cells. Both vitamin B12 and folic acid are absorbed into the body in the small bowel (small intestine). People who have had their ileum (the last part of the small bowel) removed or who have inflammation in that area can have difficulties absorbing vitamin B12 from food. This means that many people with Crohn’s, and some with Colitis, may have a vitamin B12 or folic acid deficiency. When having a vitamin B12 and folic acid test, your doctor will ask about any medicines you are taking.
Vitamin D helps your body absorb calcium and phosphate. When you have direct sunlight on your skin, your body makes vitamin D, usually in the warmer months between April and September. Vitamin D deficiency is common during the winter months. Your doctor may recommend you take vitamin D supplements or eat foods high in vitamin D, such as oily fish, red meat and egg yolks.
People with Crohn’s or Colitis may have low levels of vitamin D due to:
The body requires vitamin D to absorb calcium from food. People who do not have enough vitamin D can develop softening of the bones (osteomalacia). In children, osteomalacia is known as rickets.
Blood tests are used to check for low levels of vitamin D. If you take vitamin D supplements, your doctor may do regular tests to check that you’re taking the right dose. There are no guidelines for when to measure vitamin D. Some experts believe it should be checked once every year in everyone with Crohn’s or Colitis.
Before you start taking immunosuppressant medicine, your doctor will run tests to check for any current infections such as TB (tuberculosis), hepatitis B virus, hepatitis C virus and HIV (human immunodeficiency virus). If you haven’t had exposure to chickenpox or shingles, or had the varicella vaccine before, you should also be screened for varicella zoster virus. If you are found to have no immunity to chickenpox, you may be offered the chickenpox or shingles vaccine before you start the treatment.
If you have one of these infections, it might need to be treated before starting immunosuppressants. Screening tests are important because immunosuppressants reduce how well your immune system works, which can lead to being seriously unwell from infection.
Before starting treatment with azathioprine or mercaptopurine, you will have a blood test done to check the level of TPMT in your blood. TPMT is an enzyme that makes sure the azathioprine doesn’t stay in your body for too long. Low levels may mean the azathioprine is building up because it isn’t being taken out of your body. This can cause serious side effects such as your bone marrow not working properly. If you have low TPMT levels, the dose of azathioprine or mercaptopurine can be reduced. But if you don’t have any detectable TPMT, these medicines are not right for you, and you’ll be offered other treatments.
When you are prescribed certain medicines to treat Crohn’s and Colitis, your IBD team will use factors such as your age and weight to work out how much medicine you should be taking (the dose). Therapeutic drug monitoring is the name given to blood tests that help your IBD team measure the levels of medicine in your blood. This confirms if the dose you are being given is correct or needs changing.
Some people taking adalimumab or infliximab will have a blood test taken to see if you have developed antibodies against these medicines. Developing antibodies is a response from your immune system which leads to the medicines becoming less effective.
When you take azathioprine or mercaptopurine, your body breaks down these medicines and makes products called thiopurine metabolites. Your IBD team may ask for a blood test to measure the levels of these products in your body.
This test helps your IBD team to check that the medicine is working for you and you are taking the right dose. The results can also help your IBD team to see if you are at increased risk of side effects, such as liver problems.
Some blood tests look at how active certain genes are. The results are analysed to look for patterns that might help doctors work out if you are at high risk or low risk of getting severe inflammation. This could help your IBD team work out the most appropriate treatment for you.
At the moment, there is not much evidence to show how well these tests work, or whether they lead to better outcomes for people with Crohn’s or Colitis. Scientists are doing more research on this.
Depending on the policy where you live, these tests may be available on the NHS for people with Colitis. They are not currently available on the NHS for people with Crohn’s.
Other blood tests that may be helpful include:
For a poo test (sometimes called stool or faecal tests), you will need to collect a sample of your poo in a clean, dry screw-top container. Your doctor will provide you with the container. The NHS website has more information on how to collect and store a poo (stool) sample.
Your poo can be tested for signs of bleeding and inflammation and check whether an infection is causing diarrhoea.
If you have recently travelled abroad or had a severe flare-up, you may need extra tests to check for bacteria and infections.
Measuring the level of calprotectin (a protein contained in white blood cells) in a poo sample can show whether you have inflammation in your gut. Generally, a raised faecal calprotectin level would suggest that you should have further tests for Crohn's or Colitis. Different hospitals and clinics use different levels, but usually above 100 to 250 ug/g (micrograms of calprotectin per gram of poo) is considered a raised level.
A raised faecal calprotectin result can be caused by other conditions too, such as an infection or gastroenteritis.
The National Institute for Health and Care Excellence (NICE) recommends that faecal calprotectin tests are used in adults to distinguish between inflammatory bowel diseases (IBD), such as Crohn’s and Colitis, and other non-inflammatory conditions, such as irritable bowel syndrome (IBS). The test can also be used to check that you are responding to any medicines you are taking. Faecal calprotectin tests are sometimes used to diagnose Crohn’s or Colitis in children and young people aged under 18. As children’s levels of calprotectin are more difficult to interpret, faecal calprotectin tests in young children may only be assessed by a specialist in a hospital or clinic, rather than a GP.
Sometimes faecal calprotectin tests are used to monitor your Crohn’s or Colitis or check how well you’re responding to treatment.
Your IBD team should consider your symptoms and other test results when they suggest the best course of action for you.
The NHS has a bowel cancer screening programme for people aged 60 to 74. You use a home test kit, called faecal immunochemical test (FIT), to collect a small sample of poo and send it to a lab. The lab then checks for hidden blood in your poo. If blood shows up in your poo in the FIT test, this may be due to your Crohn’s or Colitis, rather than another condition, such as bowel cancer.
Depending on the type of Crohn’s or Colitis you have, you may have surveillance colonoscopies to check for changes in your colon and early signs of bowel cancer. See the section on colonoscopy for more information.
The FIT test can also be used to find small amounts of blood in your poo, as an alternative to a faecal calprotectin test.
An endoscopy is the general name for a test which allows a specialist doctor or nurse (an endoscopist) to use a long, thin, flexible tube called an endoscope with a small camera on the end to look closely at the lining of your gut.
The video camera sends images to a screen outside the body, so the endoscopist can see different parts of the gut.
You should receive a report of your endoscopy results within three weeks of the procedure. Contact your GP if you haven’t heard back. In some cases, you may receive your report right away, and an endoscopy nurse will explain the results to you. You may be referred for an appointment with a gastroenterologist to discuss in more detail.
Our how to get a diagnosis information explains more about the different forms of Crohn’s and Colitis, and why your endoscopy might not have found Crohn’s or Colitis.
The endoscopist will look for inflammation in certain areas of your gut. Areas of inflammation will look red, swollen or may have open sores (ulcers).
Along with looking for inflammation, the endoscopist may also:
There are several different types of endoscopies, depending on which part of the body is being examined. Read more in types of endoscopy.
The hospital or clinic staff will explain any risks or complications. They will ask you to sign a consent form to make sure you understand the risks and agree to having the test done.
In rare cases, risks and complications can include:
You will be told who to contact if you have any problems. Let your IBD team know if you have any questions or worries before the test.
The main types of endoscopy are:
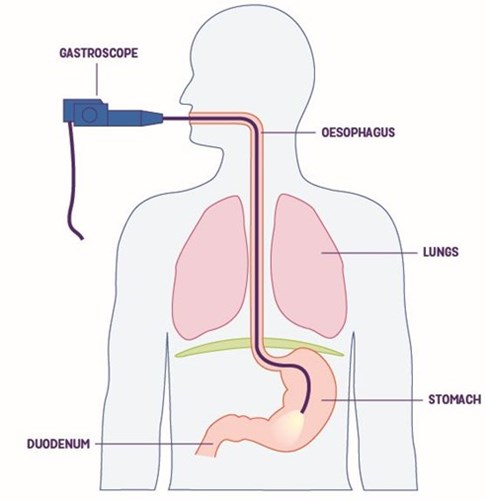
If the tube goes through your mouth, it’s called a gastroscopy or upper gastrointestinal endoscopy. The doctor will look at your throat (oesophagus), stomach, and small bowel. A gastroscopy is sometimes used to rule out Crohn’s if you have symptoms in the upper parts of your gut. It is not usually used if Colitis is suspected.
Your stomach must be empty for the endoscopist to get a clear view. You will be asked not to eat anything for at least six hours before the test. Your appointment letter should have more information but ask the hospital or clinic staff if you are unsure or have any questions.
You might be offered:
A long, thin, flexible tube called an endoscope with a small camera on the end will be gently inserted through your mouth and down your throat (oesophagus), into your stomach and the first part of the small bowel(duodenum). The specialist is looking for areas of red and swollen tissue (inflammation) and small sores called lesions.
Sedation makes you feel sleepy and relaxed, but not unconscious. You will be able to follow simple instructions during the gastroscopy. You might not remember much afterwards about the test. If you have sedation or a general anaesthetic, you will need to arrange for someone to take you home and stay with you for the next 24 hours. Sedation affects your reflexes and judgment. You must not drive, drink alcohol, operate heavy machinery, or sign important documents for 24 hours after sedation.
If you have been given throat spray, do not have anything to eat or drink until at least one hour after the gastroscopy.
Having my first colonoscopy was pretty daunting. But I needn’t have worried, as although it was uncomfortable, it was over quickly enough.
Karen
Living with Crohn’s
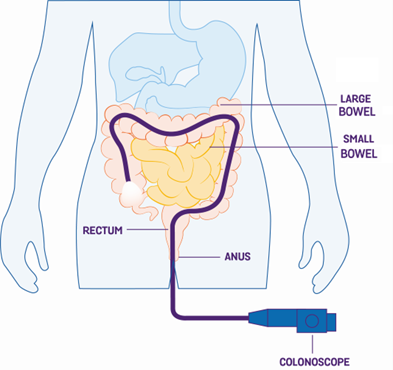
A colonoscopy is a type of examination that allows a specialist doctor or nurse to look directly at the lining of the colon and rectum using a colonoscope. This is a thin, long and flexible tube with a bright light and camera at the end.
You may feel worried or embarrassed about having a colonoscopy or the bowel preparation. It is a really important part of managing your Crohn’s or Colitis, and the colonoscopy doesn’t take long at all. Speak to your IBD team if you have any questions, or you may find it useful to look at our Facebook forum where people share their stories and experiences.
Symptoms of Crohn’s and Colitis can come and go, so your symptoms might get better while you are waiting for your colonoscopy appointment. It is still worth having your colonoscopy. Your doctor might find signs of inflammation on a colonoscopy or biopsies even when you do not have symptoms.
For a colonoscopy, your colon has to be completely clean (empty of poo). You will be asked to take a strong laxative around 24 hours before the test. This is called ‘bowel prep’. You will get a letter that will tell you what to do. The letter will either have sachets of laxatives with it for you to take or will tell you how to get them.
Once you have started taking laxatives, stay near a toilet. You will usually get diarrhoea a few hours after taking the first sachet. You may also get some abdominal cramps.
Some useful tips to help you prepare for a colonoscopy are:
The hospital or clinic will give you instructions on what to eat and drink but always ask your IBD team if you have any questions.
The tube is inserted into your bottom and travels through all of your large bowel. It’s long enough to examine the whole colon and the end of the small bowel. The specialist can check for any inflammation and whether you have any narrowed areas (strictures).
As well as looking at the lining of the bowel, the specialist may also take small pieces of bowel lining (biopsies) to examine under a microscope later. The specialist may also remove polyps (see above) to look at in more detail. The colonoscopy will usually last around 30 to 45 minutes.
To help you feel more comfortable, you may be offered:
During the colonoscopy, air is usually pumped into the bowel to help the specialist get a good view of the bowel wall. You may fart during the colonoscopy; this is completely normal so don’t feel embarrassed.
If any air remains in your bowel after the colonoscopy has finished, you may feel bloated and have some cramping. To help ease this discomfort, try walking around, eating or drinking. You may be offered a pain killer. Do not take non-steroidal anti-inflammatory medicines (NSAIDs), such as ibuprofen, unless prescribed by your doctor because they may trigger a flare-up.
You can usually go home the same day. If you have sedation or a general anaesthetic, you will need to arrange for someone to take you home and stay with you for the next 24 hours. Sedation affects your reflexes and judgment. You should avoid driving, drinking alcohol, operating heavy machinery, or signing important documents for 24 hours after sedation.
If you have questions, talk to your doctor or IBD team.
The sedative that I had for the colonoscopy made it difficult to do much afterwards. So I made sure someone came and collected me after the test, and took me home, because I needed someone to look after me.
Cari
Living with Crohn's
It is recommended that you have a colonoscopy around eight to 10 years after the start of your Crohn’s or Colitis symptoms. This is to check whether there have been any changes in your bowel. The specialist can also check for abnormal cell changes (dysplasia), which can be an early sign of bowel cancer.
You may then have follow-on colonoscopies every one, three or five years.
Due to the increased risk of developing bowel cancer for people with Crohn’s or Colitis and Primary Sclerosing Cholangitis (PSC), it is recommended that people with both conditions have a colonoscopy every year from the time of diagnosis.
See our information on bowel cancer risk.
A sigmoidoscopy is similar to a colonoscopy, but the specialist will look at part of your large bowel (rectum and beginning of the colon). Usually, a flexible endoscope is used, which is bendy and helps the specialist see further up the bowel.
Your colon needs to be completely clean (empty of poo) for the sigmoidoscopy so the specialist can get a clear view.
You will be given instructions on how to prepare for your sigmoidoscopy. You may be given laxatives or an enema.
An enema is a liquid preparation that you squirt into your bottom (anus) to soften your poo so you can easily go to the toilet. An enema can be given by yourself at home or by a nurse or doctor when you arrive at the hospital.
You will be given instructions on what you can eat and drink before and after the enema. If you have any questions, speak to the specialist or your IBD team.
The sigmoidoscopy will usually take around 10-20 minutes. It is usually done without sedation, although you may be offered gas and air (nitrous oxide). Nitrous Oxide is a medicine that you breathe in to help you relax.
During a sigmoidoscopy, the specialist may take some small samples, called biopsies, and remove small polyps.
If you have had pouch surgery, also called J-pouch surgery or ileal pouch anal anastomosis (IPAA), you may need to have the pouch examined with a sigmoidoscope to look for pouchitis (inflammation) and to check for abnormal cells (dysplasia) which can develop into cancer.
You can usually go home the same day. You may feel bloated and have some cramping in your tummy. To help ease this discomfort, try walking around, eating or drinking. You may be offered a pain killer. Do not take non-steroidal anti-inflammatory medicines (NSAIDs), such as ibuprofen, unless prescribed by your doctor because they may trigger a flare-up.
Chromoendoscopy is a technique which involves spraying special dyes onto the lining of the bowel. This is sometimes used instead of biopsies to help to find abnormal cells.
A balloon enteroscopy is an examination that uses a special endoscope with one or two small balloons at its tip. By inflating and deflating the balloons, the endoscope can be moved further into the small bowel than other types of endoscopes. The endoscope is usually inserted through your mouth or sometimes through your bottom (anus).
A balloon enteroscopy can be used to take biopsies, remove polyps and widen (dilate) strictures. Since the procedure takes longer than other endoscopies, you will usually be given a type of medicine, called a general anaesthetic, to send you to sleep.
During a capsule endoscopy, you will be asked to swallow a small capsule the size of a large vitamin pill. The capsule will travel through your gut, just like food would. The small capsule has a camera inside which is powered by tiny batteries. The camera will take photos as it passes through the gut. These photos are sent to a small data recorder, which is usually attached to a belt that you wear around your waist.
The specialist will check that the capsule is sending photos properly. You will be allowed to go home wearing the data recorder. You should avoid strenuous exercise and bending over while wearing the data recorder.
The capsule is disposable and can be flushed down the toilet. It should pass out of the body with your poo in the next day or so. Biopsies cannot be taken with the capsule. The capsule is not suitable for people with strictures or bowel obstructions as it can become stuck. Capsule endoscopy is normally used to monitor small bowel Crohn’s if MRI doesn’t show it well. It can also be used if you are suspected of having Crohn’s or Colitis and have already had a colonoscopy which returned normal results.
Before you have a capsule endoscopy, you might be asked to take a patency capsule. This is a ‘test’ capsule to check if you have any strictures or blockages which would stop the capsule from moving. The patency capsule is about the same size as the video capsule. Instead of a camera, the patency capsule has a small tag inside it. The specialist can find this tag using a scanner to see where in your gut the capsule is. If the patency capsule becomes stuck, it will dissolve into tiny pieces and pass through your gut with your poo.
X-rays and other imaging tests are used to create images of the inside of your body. The NHS website has more information on what X-rays are and how they work. Imaging tests are usually carried out by a specialist doctor, called a radiologist. Another specialist, called a radiographer, will control the scanners and machines.
X-rays and scans allow the radiologist to see images of the inside of your body. They can use these images to work out where areas of inflammation (swollen and red tissue) are in your gut, which can help diagnose either Crohn’s, Colitis or another condition.
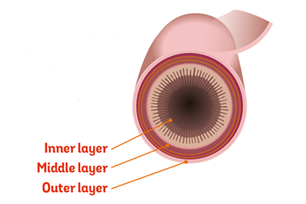
Computerised tomography (CT) and magnetic resonance imaging (MRI) scans can show which part of the bowel wall has inflammation and ulcers. Crohn’s can affect all layers of the bowel wall, while Colitis only affects the inner layer.
The hospital or clinic staff will explain any risks or complications of each test. They may ask you to sign a consent form to make sure you understand the risks and agree to have the procedure done.
In rare cases, risks and complications can include:
Being exposed to radiation can relate to a very small increase in the probability of cancer occurring many years or decades after the scan. Everyone is exposed to natural background radiation throughout daily life. This background radiation comes from naturally occurring radioactive material in the ground and atmosphere.
The UK government website has information on how much radiation you will be exposed to from each X-ray or scan, and how many days, months or years’ worth of background radiation this is equal to.
If you have any questions or are concerned about the risks, then let your doctor know.
An X-ray is taken of your tummy (abdomen) to look for areas of swollen (distended) bowel above blockages and obstructions. X-rays can also be used to diagnose toxic megacolon. Toxic megacolon is a widening or swelling of the colon that may cause a rupture (perforation). These X-rays are often used in emergency cases. They do not show as much detail of the gut as some of the other imaging tests (see below).
This x-ray is very quick to perform.
Barium is a white, chalky fluid that is not absorbed into the body but instead forms a temporary coating on the inside of the gut. Since X-rays cannot pass through barium, it is used to provide a clearer outline of the gut on X-ray pictures.
You will be asked to take barium in different ways depending on the part of the gut that is being looked at.
Barium studies have become less common because CT and MRI imaging tests are more widely available (see below).
The different types of barium tests are:
Barium swallow and meal – the radiologist will ask you to drink a mixture of barium and water while they take X-ray images of the upper part of the gut, such as the oesophagus and stomach.
Barium follow-through - you will swallow a mixture of barium and water and be asked to take a laxative the day before the test. The radiologist will take X-ray images of your stomach and small bowel as the barium passes through your gut. You will be told what to eat and drink before and after the test.
Barium enema - an enema is used to pass barium directly into your bowel through a short tube placed in the bottom (anus). Your bowel must be empty of poo before the test to make sure the images are clear. You should have instructions on what to eat and if you need to take laxatives before the test.
After taking barium, your poo will turn pale and chalky looking for a few days.
Biologic medicines are common treatments for people with Crohn’s or Colitis. Because they suppress parts of the immune system, all biologics carry an increased risk of infections such as tuberculosis (TB). Before starting biologics, you will need to have a chest X-ray to check you don’t have a latent TB infection. A latent infection is when the TB bacteria is in your body but is not active and you don’t have any symptoms. People with latent TB are not infectious. This type of x-ray is very quick to perform.
DEXA scanners use low dose X-rays to measure how dense (strong) your bones are, usually in the spine or thigh bone. This is a simple, painless test that takes around 10 minutes.
DEXA scans can show if your bones have become thinner and weaker than normal – a condition known as osteoporosis. People with Crohn’s or Colitis have an increased risk of developing osteoporosis. Having steroid treatment or low calcium levels can also increase the risk of weak bones. If you are taking steroids long-term, it is recommended that you have a DEXA scan every year. See our information on bones.
A CT scanner is a special machine that uses a series of X-ray beams to build up a detailed picture of the gut. During a CT scan, you usually lie on a moveable bed, which slowly passes through the centre of the scanner. The scanner is a ring that rotates around your body while it takes each scan. The scan is quick and painless.
You may be given a contrast dye before the scan, which helps show more detail of the gut on the scans taken. The contrast may be given in the form of a drink to swallow, an enema in your bottom or injected into a vein in your arm. You should get a letter telling you everything you need to know about the scan, including if you need to have a contrast dye.
Another type of CT scan is a CT enterography. This scan is used to look at your small bowel in more detail. Usually, you will have to drink a contrast dye before the scan, then during the scan another type of contrast dye will be injected into a vein in your arm. CT enterography scans help find inflammation, blockages and bleeding in the small bowel.
MRI scans use strong magnets and radio waves to create images of the inside of the body. MRI scans do not use X-ray radiation. The MRI scanner looks like a long tube or tunnel. You will be asked to lie very still on a moveable table, which slides slowly inside this tunnel. An MRI will usually last around 20 to 30 minutes.
You may be given a contrast dye before the scan, which helps show more detail of the gut on the scans taken.
MR enterography (MRE) is a special type of MRI. This scan is used to look at your small bowel in more detail. Usually, you will have to drink a contrast dye before the scan, then during the scan another type of contrast dye will be injected into a vein in your arm. MR enterography scans help find inflammation, blockages and bleeding in the small bowel.
The MRI scan can be noisy and make tapping sounds. You may be given earplugs or headphones to wear. The radiographer is controlling the MRI scanner from another room, but they can still see and hear you to make sure everything is going okay. If you are scared of enclosed spaces (have claustrophobia), let the radiographer know that you are worried before the test. They can offer support and help you feel more comfortable.
If you feel really anxious about having an MRI scan, you may want to ask your GP or consultant for a mild sedative; this is a medicine to help you feel sleepy and relaxed. You should arrange this before your MRI appointment.
Because MRI scanners use magnets, they are not suitable for most people who have implanted metal or electronic device, such as a pacemaker or artificial joint. Please let your team know and they can check if your implant or device is compatible and suitable for an MRI scan.
You should get a letter telling you everything you need to know about the scan, including if you need to have contrast dye.
Another type of MRI is a Magnetic Resonance Cholangiopancreatography (MRCP). This scan shows detailed images of the liver, gall bladder, bile ducts, pancreas and pancreatic ducts. An MRCP can be used to diagnose Primary Sclerosing Cholangitis (PSC).
Ultrasound is another type of scan that is used when diagnosing and treating Crohn’s or Colitis. Ultrasound scans use sound waves to create detailed images of the part of the body that the radiographer is moving the scanning probe or wand over. Ultrasound does not use X-ray radiation.
Ultrasound can show thickening of the bowel wall, abscesses and strictures.
Before the scan, you will need to drink large amounts of liquid and avoid eating for a few hours. You may be given a contrast dye before the scan, which helps show more detail of the gut on the scans taken.
You should get a letter telling you everything you need to know about the scan, including if you need to drink any contrast dye.
Endoscopic Ultrasound Scans (EUS) use a special endoscope with a tiny ultrasound transmitter in the tip. Like a normal endoscope, EUS is inserted through the mouth to examine the upper part of the gut or through the bottom (anus) to examine the colon (part of the large bowel) and ileum (the last part of the small bowel). Your doctor will be able to take small samples (biopsies) if they need to. You will usually be given a sedative or a local anaesthetic spray to numb your throat. Find out more in the section above on endoscopy.
A SeHCAT scan is used to find out whether diarrhoea is caused by bile acid malabsorption (BAM).
When you eat, bile salts (made in the liver and stored in the gall bladder) are released into the small bowel to help break down food. Normally, when bile salts reach the end of the small bowel, they are absorbed into your blood. Bile salts may not be absorbed if the ileum (last part of the small bowel) is inflamed due to Crohn’s or has been removed during surgery. Instead, bile salts enter the colon (part of the large bowel) along with high levels of water, leading to watery diarrhoea.
The SeHCAT scan involves two separate appointments. At your first appointment, you will be asked to swallow a small capsule containing a small amount of radioactive bile salts. After around an hour, a scan will be taken using a machine that can measure radioactivity. After seven days, a second scan will be done to measure the amount of radioactive bile salt still left in your body, showing whether you have problems absorbing bile salts.
There is no need to be concerned about the level of radiation since the radiation dose is low (equivalent to the amount received from natural sources of radiation in about two months). You will not need to stay away from anyone after the scan.
You should get an information sheet with your appointment letter from your hospital telling you everything you need to know about the scan.
If you have Crohn’s in the area around your bottom (perianal Crohn’s), you may be given a medicine (general anaesthesia) so that the area can be examined while you sleep. Anaesthesia is given because the examination may be too uncomfortable or painful to do while you are awake. Being asleep helps to relax the muscles in your bottom (anal sphincters and pelvic floor muscles). EUA is often used to investigate fistulas. Sometimes a special probe is used to map out the route of the fistula.
EUA is usually done as a day case, meaning you can go home the same day. If you have a general anaesthetic, you will need to arrange for someone to take you home and stay with you for the next 24 hours. Sedation affects your reflexes and judgment. You should avoid driving, drinking alcohol, operating heavy machinery, or signing important documents for 24 hours after sedation.
Studies show that pelvic magnetic resonance imaging (MRI) is more accurate than EUA at finding the course of perianal fistulas. However, EUA can still be used to assess the area. It also allows any abscesses to be drained and other treatments to be given.
We follow strict processes to make sure our information is based on up-to-date evidence and easy to understand.
Please email us at evidence@crohnsandcolitis.org.uk if:
You can also write to us at Crohn’s & Colitis UK, 1 Bishop Square, Hatfield, AL10 9NE, or contact us through our Helpline: 0300 222 5700
This page has been saved in your personal space. Go to “My Page” to view all saved pages.
We know it can be difficult to live with, or support someone living with these conditions. But you’re not alone. We provide up-to-date, evidence-based information and can support you to live well with Crohn’s or Colitis.
Our helpline team can help by:
Providing information about Crohn’s and Colitis.
Listening and talking through your situation.
Helping you to find support from others in the Crohn’s and Colitis community.
Providing details of other specialist organisations.
Please be aware we’re not medically or legally trained. We cannot provide detailed financial or benefits advice or specialist emotional support.
Please contact us via telephone, email or LiveChat - 9am to 5pm, Monday to Friday (except English bank holidays).
If you need specific medical advice about your condition, your GP or IBD team will be best placed to help.
Would you like to save the changes made to this page?
Your details were successfully saved.